U.S. drug overdose deaths are down 35% from the 2022 peak
Part of Teaching an AI Agent to Make Beautiful Charts
U.S. drug overdose deaths went up nearly every year from 1999 to 2022, climbing from 16,849 to a peak of 107,941. At the peak, that was more Americans dying of overdoses in a single year than from car crashes and gun violence combined. Then the curve broke.
CDC's final 2024 count came in at 79,384, a 26% drop in the age-adjusted death rate and the largest single-year decline CDC has tracked over the past decade. Provisional 2025 data puts the count near 70,000, about 35% below the 2022 peak. That's the first sustained two-year drop in 25 years of data. The chart below shows the full arc, including the three opioid waves that drove the rise.
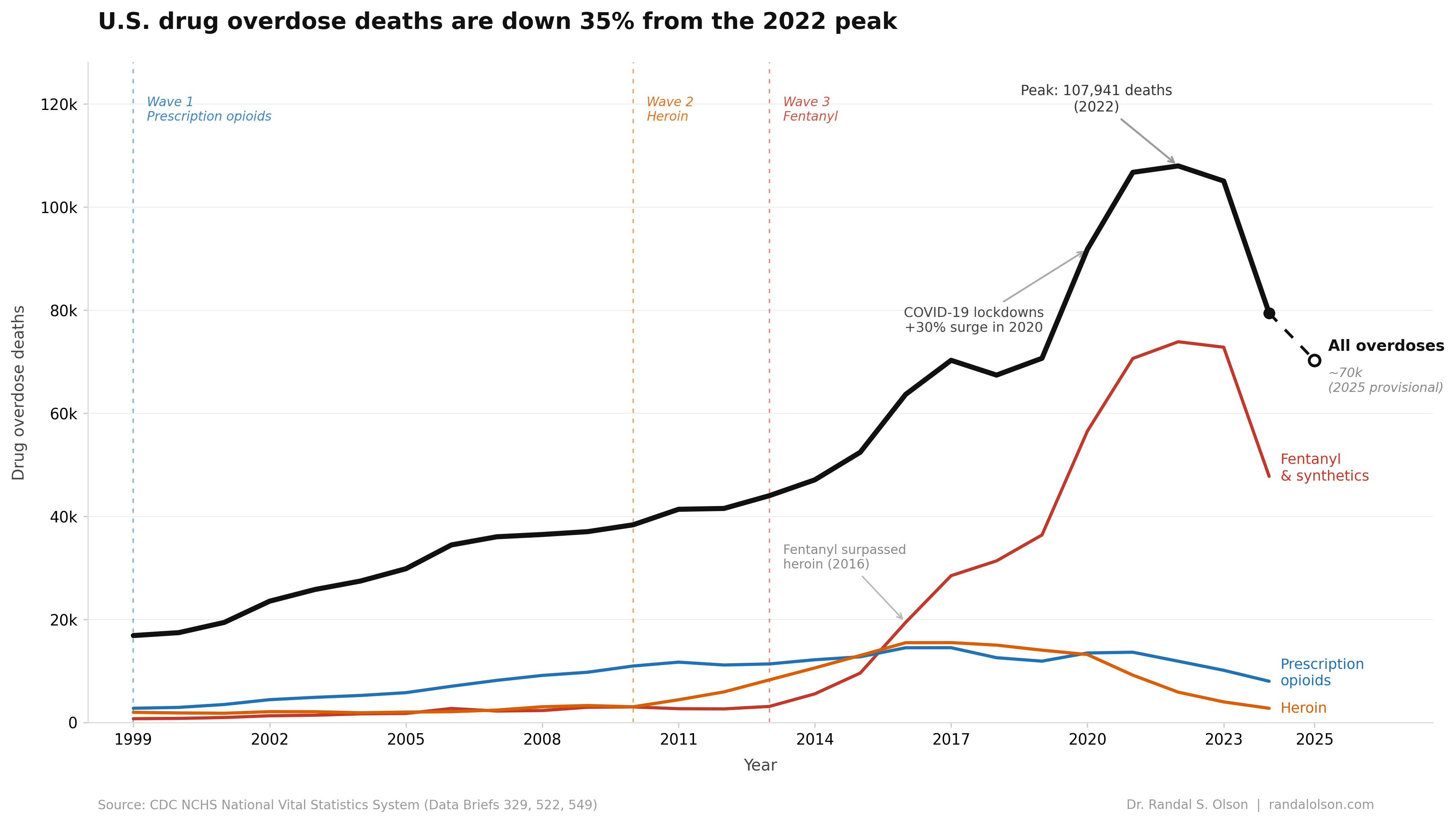
Wave 1: OxyContin flooded the market
The FDA approved OxyContin in December 1995, and it went to market in 1996. Purdue Pharma's original label included a claim that the drug's "delayed absorption...is believed to reduce the abuse liability," a statement with no clinical evidence behind it. The FDA removed the claim in 2001 after a GAO inquiry, and added a black-box warning the same year. By then, OxyContin prescriptions had jumped from 316,000 in 1996 to more than 14 million for 2001 and 2002 combined. A 2020 review in the AMA Journal of Ethics argued the deeper failure was the FDA's decision to approve OxyContin with a broad indication that let Purdue market it for everyday chronic pain.
Opioid-involved deaths tripled over those same years, from 8,050 in 1999 to 21,089 in 2010. The drugs were reaching people far beyond the severe-pain patients the label was written for, and the pipeline kept feeding the supply. Prescription opioid deaths climbed through 2011 before leveling off, but the people who had become dependent on those drugs did not disappear when prescribing tightened.
Wave 2: Heroin filled the gap
Around 2010, Purdue reformulated OxyContin to resist crushing and dissolving, cutting off a common route of misuse. Prescribers also began writing fewer opioid scripts under pressure from state and federal regulators. People who had developed opioid dependence needed a substitute, and traffickers were ready. Heroin was available and, by that point, considerably cheaper than diverted pills on the black market.
Heroin deaths jumped from 3,036 in 2010 to a peak of 15,482 in 2017. The number of past-year heroin users in the U.S. rose from 404,000 in 2002 to 681,000 in 2013 per SAMHSA's National Survey on Drug Use and Health, a shift that tracked closely with the prescription opioid crackdown. The new heroin users were mostly people already dependent on prescription opioids, switching when pills got harder to get.
Wave 3: Fentanyl reshaped the supply
Illicitly manufactured fentanyl began entering the U.S. drug supply around 2013. It is 50 to 100 times more potent than morphine, which meant traffickers could ship enormous quantities of opioid activity in a package small enough to fit in an envelope. Drug markets adapted fast. Law enforcement fentanyl seizures increased 426% from 2013 to 2014 alone, and synthetic opioid deaths climbed from 3,105 in 2013 to 73,838 in 2022.
By 2016, fentanyl had surpassed heroin as the leading driver of overdose deaths in the U.S. The reason was economic. Fentanyl is inexpensive to produce and extraordinarily potent, so it displaced heroin the way cheap imports displace domestic goods. Heroin deaths dropped steadily after 2017 because the product had changed, not because fewer people were using opioids. Per-use risk stayed high. Fentanyl's margin between a dose that produces a high and one that stops breathing is far tighter than heroin's.
COVID drove the steepest single-year jump
Overdose deaths had been rising before the pandemic, but 2020 was different. Deaths jumped 30% in a single year, from 70,630 to 91,799. Treatment access collapsed. Clinics closed or cut capacity, court-mandated programs paused, and the in-person support networks people in recovery rely on disappeared overnight. The Commonwealth Fund pointed to economic disruption, social isolation, and reduced access to treatment as the main drivers.
The 2020 surge accelerated a trajectory that was already steep. Deaths continued rising through 2021 and 2022, passing 100,000 for the first time in 2021.
What drove the two-year decline
Researchers disagree on the dominant cause. A January 2026 Science paper by Vangelov, Humphreys, Caulkins, and colleagues argued that disruptions to the fentanyl precursor supply chain out of China after a November 2023 U.S.-China summit cut potency and availability across North American drug markets, and that this supply shock did most of the work. Other researchers, including Nabarun Dasgupta at UNC, credit community-level factors, especially the explosion of community naloxone distribution. Several harm reduction programs scaled substantially over the same period. Naloxone access expanded sharply after the FDA approved an over-the-counter version in 2023, every state now has some form of Good Samaritan overdose law, and access to buprenorphine and methadone broadened through pandemic-era telehealth changes. The honest summary is that supply-side and harm reduction explanations both fit the data, and there is no consensus on the split.
The decline carried into 2025, but the pace slowed. Provisional CDC data through November 2025 put the 12-month death count near 70,000, about 12% below the 2024 final total. Humphreys warned in mid-2025 that the slowdown could mean the 2024 drop was a one-off rather than a fundamental change in the epidemic.
What the headline number leaves out
A 35% drop is real, but several pieces of the picture do not move with it.
The "deaths are down" story is overwhelmingly an opioid story. Methamphetamine-involved overdose deaths climbed from 2,266 in 2011 to 34,855 in 2023, and cocaine-involved deaths from 4,681 to 29,449 over the same period, according to CDC MMWR. Both fell in 2024 along with opioid deaths, but stimulant-involved deaths remain near record highs and the share of overdoses involving multiple drugs keeps rising.
Racial disparities are widening. Overdose death rates among Black and American Indian / Alaska Native populations have continued to rise or fall more slowly than rates among white Americans, Stateline reported. The gains have not been distributed evenly.
A new sedative is moving through the fentanyl supply. Medetomidine, a veterinary tranquilizer whose sedation cannot be reversed by naloxone, has spread fast. CDC reports of medetomidine in seized drug samples rose from 247 in 2023 to 8,233 in 2025, and across CDC sentinel testing sites in late 2025 it was detected in roughly 35% of opioid-positive samples on average, with regional pockets above 50%. The CDC issued a Health Alert Network advisory on it in April 2026.
Federal funding for the programs being credited is unstable. On January 14, 2026, the Trump administration sent termination letters wiping out roughly $1.9 billion in SAMHSA addiction and mental health grants, then reversed the cuts within 24 hours after public outcry. Broader cuts to HHS grant funding, Medicaid, and CDC data systems are still on the table. The Brookings Institution flagged the trajectory as a real threat to the durability of the trend. Even after the 35% drop, roughly 70,000 Americans still died of an overdose in 2025, more than double the count from a decade earlier.
How this chart was made
An AI agent built this chart end-to-end as part of the Beautiful Charts with AI series. It researched the data, built the chart in Python, and iterated on the design until it passed the Tufte Test, a data visualization quality standard built by Goodeye Labs on Truesight.
Data source: CDC NCHS Data Briefs 329, 522, and 549, covering final overdose death counts 1999 through 2024. The 2025 provisional data point uses the CDC VSRR predicted 12-month count through November 2025, available at data.cdc.gov. The full dataset used for this chart is available here.
Beautiful Charts with AI
Want to test your own charts against the same quality bar?
Try the Tufte Test on your own chart, or get future updates on AI evaluation and chart quality from Goodeye Labs.

Dr. Randal S. Olson
AI Researcher & Builder · Co-Founder & CTO at Goodeye Labs
I turn ambitious AI ideas into business wins, bridging the gap between technical promise and real-world impact.